Peer pressure can be tough for kids to resist, even if it comes from robots.
School-aged children tend to echo the incorrect but unanimous responses of a group of robots to a simple visual task, a new study finds. In contrast, adults who often go along with the errant judgments of human peers resist such social pressure applied by robots, researchers report August 15 in Science Robotics.
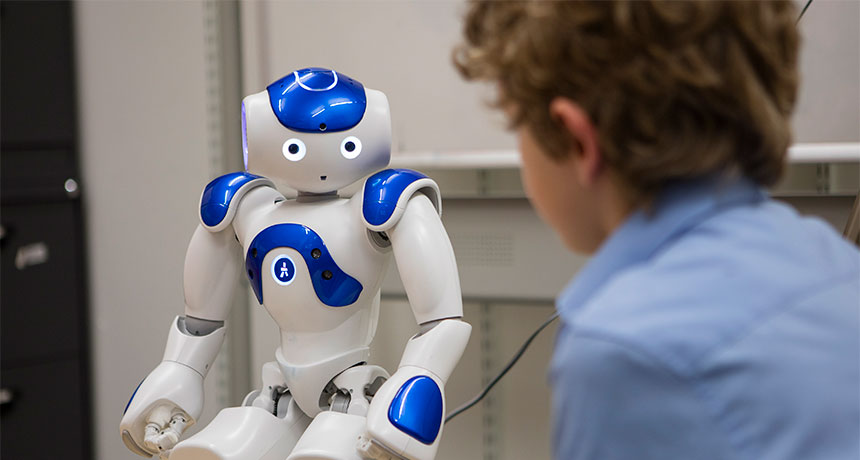
“Rather than seeing a robot as a machine, children may see it as a social character,” says psychologist Anna-Lisa Vollmer of Bielefeld University, Germany. “This might explain why they succumb to peer pressure [applied] by robots.” Little is known about how either adults or children respond to the behavior of lifelike robots designed to interact with people, for example, as museum tour guides, child-care assistants and teaching aids.
In a preliminary examination of the influence of social robots, Vollmer’s group adapted a 1950s social psychology experiment in which most adults agreed with groups of peers who had been coached to say that lines of different lengths were in fact the same length (SN Online: 5/15/18).
Vollmer’s team observed comparable social conformity in a study of 60 British adults, ages 18 to 69, who judged line lengths after hearing the opinions of three peers who were working with the researchers. Participants usually endorsed peers’ unanimous, inaccurate judgments. Conformity vanished, however, when volunteers performed the task while sitting with three robots that, on some trials, agreed on an incorrect answer. Each robot was programmed to make periodic movements, such as blinking its eyes and briefly gazing at others. Robots spoke with distinctive, individualized voice pitches when making line judgments. When children sat with the robots, though, the kids frequently went all-in. The study’s 43 participating British grade-schoolers, aged 7 to 9, agreed with three-quarters of the robots’ unanimous, inaccurate answers. The kids did not participate in conformity experiments with trios of same-age human peers, given the difficulty of getting youngsters to act convincingly according to researchers’ directions.
Still, larger samples of volunteers are needed to confirm that kids usually cave to social pressure from robots. Cultural factors, such as being raised in a society that emphasizes individualism or group values, also may influence how people of all ages perceive and react to social robots.
Three unresolved issues in particular stand out, says psychologist and child development researcher Paul Harris of Harvard University. First, it’s unclear whether some robot behaviors, but not others, triggered conformity in children. A bot’s periodic head turns toward a child, for example, might sway that youngster’s choice more than the same robot’s eye blinks or finger movements. It’s also unclear why adults who bent to human peer pressure reversed course with robots.
Finally, Harris asks, “Would fine-tuning of the robots’ repertoire [of movements and vocalizations] eventually elicit deference even from adults?”
Experimental anticancer drugs may help protect against liver damage caused by acetaminophen overdoses.
In mice poisoned with the common painkiller, the drugs prevented liver cells from entering a sort of pre-death state known as senescence. The drugs also widened the treatment window: Mice need to get the drug doctors currently use to counteract an overdose within four hours or they will die, but the experimental drugs worked even 12 hours later, researchers report August 15 in Science Translational Medicine. If the liver-rescuing results are verified in clinical trials, this therapy may buy time for people who accidentally or intentionally overdose on Tylenol or other medications containing the painkiller acetaminophen. In the United States, such overdoses occur more than 100,000 times a year and are the leading cause of acute liver failure. Many people get treatment on time or recover on their own, but some require emergency liver transplants. And 150 people on average die of acetaminophen poisoning each year.
Currently, doctors treat such overdoses with N-acetylcysteine, an antidote that must be given within eight hours of ingesting a potentially fatal dose. Some people don’t make it to a doctor in time, and will die or need transplants.
In the study, untreated mice died within 18 hours. But mice given the new drugs survived at least a week until researchers sacrificed the rodents to examine their livers.
The anticancer drugs work by blocking a signal from a tumor growth-stimulating protein called TGF-beta, which is activated by inflammation provoked by the overdose. When unchecked, TGF-beta sends a stress signal that puts liver cells in senescence, liver specialist Thomas Bird of Cancer Research UK Beatson Institute in Glasgow and colleagues report.
Freshwater is crucial for drinking, washing, growing food, producing energy and just about every other aspect of modern life. Yet more than 2 billion of Earth’s 7.6 billion inhabitants lack clean drinking water at home, available on demand.
A major United Nations report, released in June, shows that the world is not on track to meet a U.N. goal: to bring safe water and sanitation to everyone by 2030. And by 2050, half the world’s population may no longer have safe water.
Will people have enough water to live?
Two main factors are pushing the planet toward a thirstier future: population growth and climate change. For the first, the question is how to balance more people against the finite amount of water available. India has improved water access in rural areas, but remains at the top of the list for sheer number of people (163 million) lacking water services. Ethiopia, second on the list with 61 million people lacking clean water, has improved substantially since the last measurement in 2000, but still has a high percentage of total residents without access.
Short of any major but unlikely breakthroughs, such as new techniques to desalinate immense amounts of seawater (SN: 8/20/16, p. 22), humankind will have to make do with whatever freshwater already exists.
Most of the world’s freshwater goes to agriculture, mainly to irrigating crops but also to raising livestock and farming aquatic organisms, such as fish and plants. As the global population rises, agricultural production rises to meet demand for more varied diets. In recent decades, the increase in water withdrawal from the ground or lakes and rivers has slowed, whether for agriculture, industries or municipalities, but it still outpaced the rate of population growth since 1940. That means every drop is increasingly precious — and tough choices must be made. Plant your fields with sugarcane to make ethanol for fuel, and you can’t raise crops to feed your family. Dam a river to produce electricity, and people downstream can no longer fish. Pump groundwater out for yourself, and your neighbor might just want to fight over it. Researchers call this the food-water-energy nexus and say it is one of the biggest challenges facing our increasingly industrialized, globalized and thirsty world.
“There just isn’t enough water to meet all our needs,” says Paolo D’Odorico, an environmental scientist at the University of California, Berkeley whose team analyzed the food-water-energy nexus in a paper published online April 20 in Reviews of Geophysics.
Overall, the energy sector is expected to consume more and more water in decades to come. And sometimes what sounds like a good idea — such as switching to renewable energy sources to reduce carbon emissions — might help in one area but hurt in another. For example, it can take more water to grow biofuel crops than to consume fossil fuels. ** Water consumption is defined as water that is used and not returned to its source. These projections are based on nations’ stated commitments to phase out fossil fuel subsidies and reduce emissions of greenhouse gases.
Source: World Energy Outlook 2016 Special Report: Water-Energy Nexus/IEA
Then there’s climate change. As greenhouse gases build up in Earth’s atmosphere, trapping heat and altering the planet’s weather and climate, water will become more precious. Rising global temperatures alter weather patterns and change how water cycles between the ground and the atmosphere. Freshwater stores can shrink. Extreme events, such as flooding and drought, are becoming more common on our warming planet (SN: 1/20/18, p. 6). That means more water in places where people don’t need it, and less water where they do.
The map below shows how water stress — the ratio of water use to water supply — is expected to look by the year 2040. It assumes a “business-as-usual” scenario in which carbon emissions rise steadily. The highest stress is expected in areas where water supply is vulnerable because of already arid climates and growing populations. Cities will bear the brunt of future water shortages. Early this year, it looked as if the more than 4 million people living in Cape Town, South Africa, were going to run out of water. Officials calculated a “Day Zero” in April when the taps would run dry. Only through belated and desperate conservation measures, such as slashing the amount of water for irrigating crops, did city residents eke through until the rainy season began in May. That Cape Town crisis is almost certainly the first of many.
By 2050, some 3.5 billion to 4.4 billion people around the world will live with limited access to water, more than 1 billion of them in cities. Among 482 cities, more than a quarter will face demands that outpace supply, according to a study that analyzed water sources and demands. In general, urban growth is the main driver of cities’ future water deficits. Los Angeles tops the list because its population is expected to boom even as climate change dries up its water sources. Cities will be worse off if other sectors get priority for water access. In the face of such inexorable changes, it’s easy to despair. But science offers hope, in the form of alternative paths forward. Computer modelers at MIT, for example, find that policies to fight climate change, such as the 2015 Paris agreement that the United States announced its intention to pull out of last year (SN Online: 6/1/17), can reduce the severity of future water shortages. If nations follow commitments similar to those in the agreement, 60 million people across Asia could avoid dire water scarcity by 2050, the team wrote in June in Environmental Research Letters.
But the Paris agreement is not enough. As research increasingly makes clear, there are trade-offs and decisions to be made. Cape Town’s experience shows how governments need to better prepare for the competing demands on water supplies. Municipalities may need to raise the cost of water to the point where people value it enough to conserve it.
“We can address the problem by thinking about technological solutions, but we also have to think about changing our behavior,” says Martina Flörke, a hydrologist and environmental scientist at the University of Kassel in Germany. “If we can make clear … that water has value, that it’s an ecosystem service that we use and have to take care of — then we are really thinking about how to adapt.”
Here’s good news for anyone who’s had to sweep up pasta shards after snapping dry spaghetti and thought, “there’s got to be a better way.”
There is.
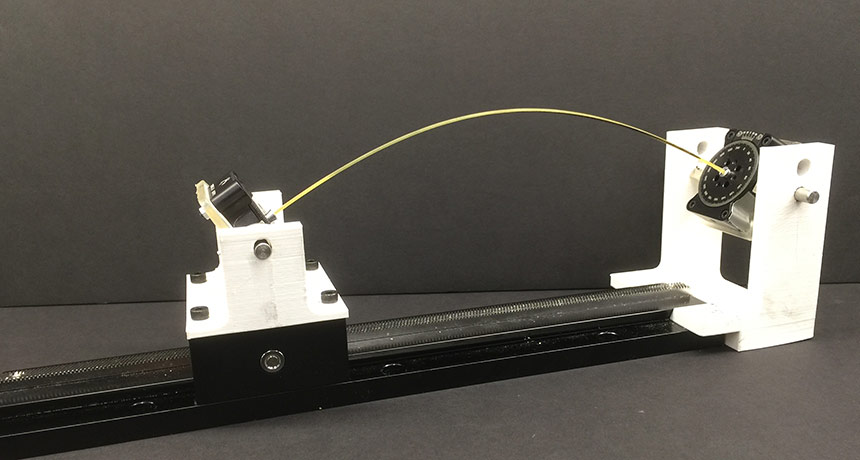
Simply bending a stick of spaghetti in half typically shatters it into three or more fragments. That’s because when the stick breaks, vibrations wrack the remaining halves, causing smaller pieces to splinter off (SN: 11/12/05, p. 315). To avoid this problem, give the spaghetti stick a twist before bending it, researchers report online August 13 in Proceedings of the National Academy of Sciences. Vishal Patil, a mathematician at MIT, and colleagues discovered this technique by breaking hundreds of pieces of pasta with a custom-made spaghetti-snapping device. These observations, along with computer simulations of the system, reveal that when a spaghetti stick is twisted, it doesn’t bend as far before breaking. As a result, the vibrations that rattle the spaghetti halves post-snap aren’t strong enough to cause further fracturing.
The exact amount of twist required to give pasta a clean break depends on the length of the rod, but for a typical stick 24 centimeters long to crack neatly in two, it’s at least 250 degrees.
This strategy may not be much practical help in the kitchen; Patil and colleagues aren’t selling their spaghetti snapper for $19.95 — and even if they were, meticulously twisting and bending pieces of pasta one-by-one is hardly efficient meal prep. Still, the discovery of the bend-and-twist technique may lend new insight into controlling the breakage of all kinds of brittle rods, from pole vault sticks to nanotubes.
Half a century ago, if you asked any teenage science fan to name the best popular science writers, you’d get two names: Isaac Asimov and George Gamow.
Asimov was prominent not only for his nonfiction science books, but also for his science fiction. Gamow was known not only for writing popular science, but was also a prominent scientist who had made important contributions both to physics and biology.
Fifty years ago this month, Gamow’s career ended when he died at the age of 64. His books and scientific papers survive him, leaving plenty of science and science writing worth celebrating. Nuclear physics, astrophysics, modern cosmology and molecular biology all benefited from Gamow’s fertile intellect. Like Asimov, Gamow was born in Russia (Odessa). But while Asimov came to the United States as a child, Gamow grew up in Russia, went to college first in Odessa (studying math) and then to the university in Petrograd (soon to become Leningrad), where he became a physicist. At Leningrad he attended lectures by the mathematician Alexander Friedmann. Friedmann was the first to fully realize that Einstein’s new general theory of relativity implied a dynamic universe — one that would expand or contract — rather than the static never-changing cosmos that most experts (including Einstein) believed in at the time.
Gamow planned to pursue a career in relativity under Friedmann’s direction. But Friedmann died young, in 1925. So Gamow fell in with a group of students more interested in quantum physics than relativity. “We spent all our time following the new [quantum] publications and trying to understand them,” Gamow wrote in his autobiography.
While a visitor at one of Europe’s top centers for quantum theory — the University of Göttingen in Germany — he solved a mystery about radioactive decay by identifying one of the quantum world’s most important phenomena: tunneling. In one form of radioactive decay, an atomic nucleus emits alpha particles that are moving too slowly to have overcome an energy “barrier” supposedly preventing their escape. (The analogy is a hill too steep for a slow-moving ball to reach the top without rolling back down.) Gamow showed that the wave mechanics version of quantum physics permitted the alpha particle to “tunnel” through the energy-barrier hill. Quantum tunneling turned out to be important for many other features of nature, such as how the sun shines, how many chemical reactions proceed and maybe even how the universe began. His work on tunneling impressed Niels Bohr, the leading quantum physicist in the world, earning Gamow a fellowship for study at Bohr’s Institute for Theoretical Physics in Copenhagen. During time there and at Cambridge University, Gamow became one of the world’s leading experts on nuclear physics theory. He also became well-known for his humor and irreverence, including a “relentless mockery of science’s solemnity,” as one biographical account put it. Returning to the Soviet Union in 1929, Gamow found the political atmosphere for continuing his work unfavorable. He eventually managed to emigrate to the United States, where he obtained a position at George Washington University in Washington, D.C., in 1934. There he studied the evolution and energy production of stars, producing fruitful insights into the stellar explosions known as supernovas. Later, he turned his attention to the universe at large, developing early versions of what became the Big Bang theory (Gamow didn’t like the name) of the origin and evolution of the universe. In 1942, the historian Helge Kragh wrote, “Gamow clearly endorsed a big-bang picture and suggested that the gross material of the present world is the result of what happened some two billion years ago in a highly compressed primeval state.” Gamow’s timing was off (it was nearly 14 billion years ago), but his basic idea was right. After World War II, Gamow found new fun with the “physics of biology.” He wondered, for instance, about the physical processes allowing cells to make proteins. Inspired by Watson and Crick’s 1953 paper on the structure of DNA — the molecule that makes genes — Gamow speculated that some sort of code could be translated from DNA to build the long chains of amino acids that constituted proteins. Nature provided merely 20 such amino acids for constructing thousands of distinct proteins.
Gamow realized that DNA’s four subcomponent “bases” could be thought of as numbers that could be translated into “words” specifying a chain of amino acids, linked in a specific order, chosen from their 20-letter “alphabet.” He saw that if you chose three DNA bases at a time, there were about 20 possible combinations, indicating that each three-base “triplet” might correspond to an amino acid. He couldn’t crack the code for which base combinations went with which amino acids, though, even with help from some U.S. Navy cryptologists. But Gamow had more or less the right idea, although he didn’t recognize at first that an intermediate molecule, RNA, had to “read” the DNA code first before transferring the information to the cell’s protein-making apparatus.
Throughout his career, Gamow desired to share his enthusiasm for the science he investigated, not only with fellow scientists but with people in general. Today, it is fairly common for prominent scientists to write popular books. But it was not that way in the 1930s, when Gamow first tried to explain relativity and quantum physics through the eyes of his fictional character, Mr. Tompkins. Mr. Tompkins lived in worlds where the speed of light was small or Planck’s constant was large, allowing Gamow to illustrate the strangeness of the new physics in an entertaining and intuitively accessible way. To learn about Heisenberg’s uncertainty principle, for instance, Mr. Tompkins visited a billiard parlor where a professor placed a ball inside a wooden triangle. The ball began to move rapidly at varying speeds within the triangle, because restricting its position to the triangular space increased the uncertainty about its velocity. (And then the ball escaped the triangle, not by jumping over its wooden wall, but by “leaking” through it. Tunneling.)
After many rejections, Mr. Tompkins in Wonderland appeared in 1940, followed by Mr. Tompkins Explores the Atom in 1944. Later Gamow produced other more straightforward accounts of the frontiers of physics, and science more generally, in such books as One Two Three … Infinity and Matter Earth and Sky.
Gamow moved to the University of Colorado in 1956, focusing on his popular books as his prominence in science diminished. His nonconformity and irreverent attitude, along with his emphasis on popularization, did not play well with many of his peers. And he was a heavy drinker, impairing his ability to engage with other physicists and possibly contributing to his death.
Still, his science was substantial. And even if it hadn’t been, his writing contributed to the scientific enterprise via another important avenue — by opening the wonders of the world of science to a great many teenagers who are scientists, or science writers, today.
A scientific takedown of a famous finding known as the 30-million-word gap may upend popular notions of how kids learn vocabulary.
Research conducted more than 20 years ago concluded that by age 4, poor children hear an average of 30 million fewer words than their well-off peers. Since then, many researchers have accepted the reported word gap as a driver of later reading and writing problems among low-income youngsters. A Providence, R.I., program inspired by the study, for example, now teaches poor parents how to talk more with their kids. But here’s the rap on the word gap: It doesn’t exist, says a team led by psychologist Douglas Sperry of Saint Mary-of-the-Woods College in Indiana. In a redo of the original study, virtually no class differences appeared in the number of words addressed to young children by a primary caregiver, Sperry and colleagues report in a study to be published in Child Development.
What’s more, after including speech spoken directly to children by various caretakers as well as family members’ conversations that the youngsters could easily overhear, kids in some poor and working-class communities heard more words on average than middle-class youngsters, the scientists say. Within each of those communities, some children heard many more words than others did despite belonging to the same social class, Sperry’s team adds.
“It’s time to turn a skeptical eye to the word-gap claim,” Sperry says.
Researchers usually treat word learning as a product of one or both parents regularly talking to a child. But different, equally effective ways exist for children to learn vocabulary, Sperry contends. Depending on culture and community, word learning depends to varying extents on a main caretaker talking to a child, many caretakers talking to a child and youngsters overhearing family members talking, he says (SN: 2/17/18, p. 22). The original word-gap study included 42 children in Kansas from either of four communities — poor, working class, middle class or wealthy professional. Sperry’s group analyzed data on word use collected during home observations of 42 children in five communities — poor whites in South Baltimore, poor blacks in Alabama, working-class (largely blue-collar) whites in Indiana and Chicago, and middle-class (largely white-collar) whites in Chicago. Videotaped home observations began when children were 18 to 30 months old. Intermittent observations continued until kids reached ages 32 to 48 months. Most primary caregivers were children’s mothers.
Primary caregivers in poor, black Alabama families directed an average of 1,838 words per hour to their children, close to the corresponding figure of 2,153 words per hour for high-income, white caregivers in Kansas in the original word-gap study. The earlier study reported that primary caregivers on welfare in Kansas spoke an average of 616 words per hour to their children, about one-third the total spoken to poor, black children in the new study. Primary caregivers from working-class and middle-class families in the new study uttered an average of 1,048 to 1,491 words per hour to youngsters.
Taking multiple caregivers into account, average hourly words spoken to children in each community increased by 17 percent or more. An increase of 58 percent occurred in Alabama’s poor, black households. In addition, kids in poor families overheard an average of 3,203 words per hour. Eavesdropping figures reached no higher than about 2,500 words per hour in the other households. Greater numbers of older siblings in the poor, black families contributed to that disparity, the researchers suspect.
The new study convincingly rejects claims of a word-gap for poor children, says cultural anthropologist Jennifer Keys Adair of the University of Texas at Austin.
White, middle-class parents and many educators wrongly assume that vocabulary learning always proceeds best via one-on-one interactions of parents with children, or teachers with grade-school students, Adair says. That assumption may not apply to kids from other cultural backgrounds. Adair has found, for instance, that first-graders from Latin American immigrant families — who were allowed to devise classroom projects, collaborate with one another and ask questions without raising their hands — did especially well three years later on state English assessments.
But some child researchers say the new study falls short of showing that poor kids are generally exposed to as much language as better-off peers.
Sperry’s group, for example, did not study children in upper-class, professional households, as researchers did in the 1990s. And other studies of early word learning point to a need for programs that help low-income parents engage their children in language-boosting conversations, conclude psychologist Roberta Golinkoff of the University of Delaware in Newark and colleagues in comment that will appear in the same journal.
“Overhearing language about death and taxes — topics of interest to adults — can never be as effective for language learning as participating in conversations about what matters to children,” Golinkoff and her colleagues write in their comment.
Kids frequently eavesdrop, Sperry responds. Ongoing research shows that “young children are very interested in talk that occurs around them, particularly when parents or siblings are talking about the child.”
While that may be so, little is known about the role of overheard speech and social context in language learning. Sperry and his colleagues plan to take a closer look at the difficult-to-study issue of how eavesdropping on family members influences later reading and writing skills.
Late-night comedians skewered Vice President Mike Pence in August when he announced preliminary plans for a new branch of the U.S. military dubbed the “Space Force.” Jimmy Kimmel likened the idea to a Michael Bay action movie, while Jimmy Fallon quipped that the Space Force’s chain of command would go “E.T., Yoda, then Groot.”
But, as a new book by astrophysicist Neil deGrasse Tyson and researcher-writer Avis Lang demonstrates, the militarization of space is no joke. In Accessory to War, Tyson and Lang chronicle how war-makers have long wielded knowledge of outer space as a weapon. This bloody history features Christopher Columbus exploiting his awareness of an upcoming lunar eclipse to threaten natives on the island of Hispaniola with divine retribution, as well as the United States using satellite intelligence to fight the Gulf War.
“As for America’s forthcoming wars,” Tyson and Lang predict, “they will be waged with even more formidable space assets.”
But just as militaries have long used space science and space-based technology to their advantage, astronomers and astrophysicists have reaped the rewards of military investment. James Cook, a captain in the British Navy, for example, established an observatory in Tahiti. Observations of Venus passing across the face of the sun in 1769 from that observatory helped astronomers pin down the distance between Earth and the sun. During the Cold War, U.S. military satellites designed to watch for nuclear detonations discovered gamma-ray bursts, some of the most spectacular explosions in the universe (SN: 1/10/15, p. 15). Tyson and Lang’s millennia-long world history is sprawling. The book is exhaustively researched, almost to the point of information overload. It’s easy to get bogged down in parenthetical asides about minor characters or paragraph-long lists. The book is the antithesis of Tyson’s starry-eyed, bite-sized Astrophysics for People in a Hurry and may end up on the shelves of more history buffs than astro nerds.
Still, Accessory to War lives up to much of the promise of a Neil deGrasse Tyson read: Written from Tyson’s perspective, the narration is rich with wry humor and vivid descriptions of cosmic goings-on. For anyone who is, like Tyson, “smitten by the cosmos,” the book is a stark reminder that astrophysics has been both a benefactor and beneficiary of human conflict — and that the final frontier will likely be the battleground of many future skirmishes.
Buy Accessory to War from Amazon.com. Science News is a participant in the Amazon Services LLC Associates Program. Please see our FAQ for more details.
Perhaps the most unsettling scene in Poached, by science journalist Rachel Love Nuwer, comes early in the book, in a fancy restaurant in Ho Chi Minh City, Vietnam. The author and two friends sit down and are handed leather-bound menus offering roasted civet, fried tortoise, stewed pangolin and other delicacies made from rare or endangered species. The trio makes an abrupt exit, but only after seeing a live cobra gutted at one table and a still-living civet brought out to feed another group of diners. Statistics on the illegal wildlife trade can be mind-numbing. Rhinos have dwindled to just 30,000 animals globally and tigers to fewer than 4,000. Over a million pangolins — scaly anteaters found in Africa and Asia — have been killed in the last 10 years. Just last month came a report from the Humane Society of the United States and the Humane Society International that the United States imported some 40,000 giraffe parts, from about 4,000 animals, between 2006 and 2015.
But in Poached, Nuwer gives readers a firsthand view of what the illegal wildlife trade is like on the ground and what, if anything, can be done to stop it. She accompanies a poacher into the U Minh forest of Vietnam in search of water monitors, cobras and civets. (Thankfully, they don’t find any.) She has dinner with a man who keeps a rhino horn in an Oreo tin. She visits a zoo in Japan that may have helped popularize trade in the rare earless monitor lizard. And she attends numerous meetings of wildlife officials and conservationists as they attempt to fight back against the illegal trade.
Poached isn’t all gloom and doom; there are a few success stories. Nuwer, for instance, visits Zakouma National Park in Chad where managers have halted the slaughter of elephants. This hard-won accomplishment exemplifies the book’s underlying message: There are no easy solutions to stopping wildlife trafficking. The effort in Zakouma required a lot of money and training for its rangers, which is not available in most places.
What’s most needed, Nuwer argues, is changing how we think about wildlife crime. Many people view poaching as belonging to a special category of illegal activity. But it’s not; it’s just crime. Those involved are often also dealing in drugs or conflict diamonds or human trafficking. A change in mind-set could help overcome a major conservation obstacle, Nuwer notes. Rather than detectives and the courts being tasked with handling this sort of crime, the job has been left to rangers, wildlife managers and conservationists. “As some have put it,” she writes, “it is like asking botanists to stop the cocaine trade.” The world’s wildlife deserves better than that.
A strand of spaghetti snaps easily, but an exotic substance known as nuclear pasta is an entirely different story.
Predicted to exist in ultradense dead stars called neutron stars, nuclear pasta may be the strongest material in the universe. Breaking the stuff requires 10 billion times the force needed to crack steel, for example, researchers report in a study accepted in Physical Review Letters.
“This is a crazy-big figure, but the material is also very, very dense, so that helps make it stronger,” says study coauthor and physicist Charles Horowitz of Indiana University Bloomington. Neutron stars form when a dying star explodes, leaving behind a neutron-rich remnant that is squished to extreme pressures by powerful gravitational forces, resulting in materials with bizarre properties (SN: 12/23/17, p. 7).
About a kilometer below the surface of a neutron star, atomic nuclei are squeezed together so close that they merge into clumps of nuclear matter, a dense mixture of neutrons and protons. These as-yet theoretical clumps are thought to be shaped like blobs, tubes or sheets, and are named after their noodle look-alikes, including gnocchi, spaghetti and lasagna. Even deeper in the neutron star, the nuclear matter fully takes over. The burnt-out star’s entire core is nuclear matter, like one giant atomic nucleus.
Nuclear pasta is incredibly dense, about 100 trillion times the density of water. It’s impossible to study such an extreme material in the laboratory, says physicist Constança Providência of the University of Coimbra in Portugal who was not involved with the research. Instead, the researchers used computer simulations to stretch nuclear lasagna sheets and explore how the material responded. Immense pressures were required to deform the material, and the pressure required to snap the pasta was greater than for any other known material.
Earlier simulations had revealed that the outer crust of a neutron star was likewise vastly stronger than steel. But the inner crust, where nuclear pasta lurks, was unexplored territory. “Now, what [the researchers] see is that the inner crust is even stronger,” Providência says.
Physicists are still aiming to find real-world evidence of nuclear pasta. The new results may provide a glimmer of hope. Neutron stars tend to spin very rapidly, and, as a result, might emit ripples in spacetime called gravitational waves, which scientists could detect at facilities like the Advanced Laser Interferometer Gravitational-wave Observatory, or LIGO. But the spacetime ripples will occur only if a neutron star’s crust is lumpy — meaning that it has “mountains,” or mounds of dense material either on the surface or within the crust.
“The tricky part is, you need a big mountain,” says physicist Edward Brown of Michigan State University in East Lansing. A stiffer, stronger crust would support larger mountains, which could produce more powerful gravitational waves. But “large” is a relative term. Due to the intense gravity of neutron stars, their mountains would be a far cry from Mount Everest, rising centimeters tall, not kilometers. Previously, scientists didn’t know how large a mountain nuclear pasta could support.
“That’s where these simulations come in,” Brown says. The results suggest that nuclear pasta could support mountains tens of centimeters tall — big enough that LIGO could spot neutron stars’ gravitational waves. If LIGO caught such signals, scientists could estimate the mountains’ size, and confirm that neutron stars have superstrong materials in their crusts.
Mayflies swarming a central Pennsylvania bridge over the Susquehanna River are a good thing, and a bad thing. Before the 1972 Clean Water Act, the river was too polluted to support the primitive aquatic insects. So their comeback is a sign that the water is healthier, says forensic entomologist John Wallace of nearby Millersville University.
But those swarms have become a nighttime menace for people driving or walking across the Columbia-Wrightsville bridge — thanks to the 2014 installation of large, 1930-era lamps along the two sides of the bridge. Soon after the lights were added, adult mayflies of the species Hexaginia bilineata began invading — causing blizzard-like conditions on the 2-kilometer overpass. The swarms were so intense in 2015, the bridge was closed following three accidents, and bulldozers were brought in to remove knee-deep piles of insect carcasses. Local officials have since tried to cope by occasionally turning off the lights, but this is problematic on a high-traffic bridge, says Wrightsville borough president Eric White. So Wallace was called in this year to make sense of the mayfly madness.
Wallace says he and undergraduate student Marisa Macchia have been collecting specimens from both sides of the bridge, and “comparing the mayfly abundance and diversity when lights are on versus when lights [are] off.” The researchers are trying to determine the swarm density per hour from the start of the emergence to the end. As larvae, mayflies drift downstream with the water current, Wallace says. When the adults emerge from the water, they fly upriver, following the water’s moonlit path of polarized light. At the end of their adult life spans of 24-48 hours, the insects mate and the females drop to the water’s surface — dying while releasing their eggs to the silt below. But that bridge, with those lamps, is breaking that path of polarized light, luring the mayflies up to the structure and causing the confused insects to perform their “drop, deposit and die” routine on the road.
“Any human light … car light, street light — are examples of unpolarized light,” Wallace says. But when reflected off asphalt or car paint, it resembles the river’s polarized light.
Wallace’s research will inform blueprints for renovating the historic bridge, White says. The goal is ultimately to guide the mayflies back to the river’s surface.